Part 1
Two orthogonal views of the same injured leg with soft tissue and bone defects which cannot be easily replaced.


Above knee amputation is realistic option but function of the limb after the amputation is not as good as someone would expect.
Amputation is certainly our last option.
CT images below speak for themselves. Significant open fracture with gas around bone and soft tissue defect which required massive free flap.

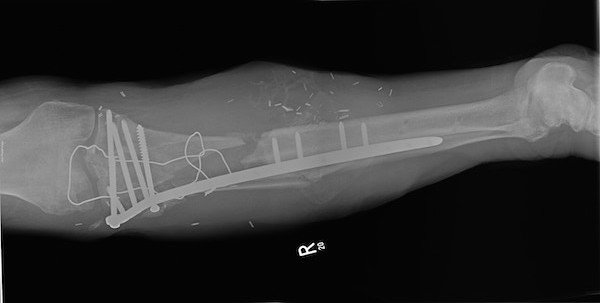
Front view after fixation of fracture and reconstuction of extensor mechanism with cerclage wire.

Side view post fracture fixation and filling of a “gap” with bone cemented with antibiotics.
Injury happened 9 months ago.
After soft tissue reconstruction with a free flap and temporary external fixatour bone fragments were fixed with a locking plate and defect filled with a bone cement mixed with bone substitute loaded with antibiotics.
Extensor mechanism defect due to the loss of patellar ligament attachment was reconstructed using a wire.
Unstable lateral corner (this was not just “simple” PLC instability) was fixed with a 6.5mm screw through the fibula’s head and knee “stability” was regained.
After couple of months bone cement was removed and second stage of Masquelet procedure was carried out. During the second stage of Masquelet foreign body membrane was identified, opened and bone graft was inserted into confined space. Antibiotics in antibiotic carrier were added and membrane was closed.

Front view post removal of cement and bone grafting.

Side view post removal of cement spacer and RIA bone grafting
Unstable lateral corner (this was not just “simple” PLC instability) was fixed with a 6.5mm screw through the fibula’s head and knee “stability” was regained.
After couple of months bone cement was removed and second stage of Masquelet procedure was carried out. During the second stage of Masquelet foreign body membrane was identified, opened and bone graft was inserted into confined space. Antibiotics in antibiotic carrier were added and membrane was closed.
Unfortunately bone became infected with patient becoming properly septic after second stage of Masquelet procedure has been done. Additional surgical debridement with removal of bone graft and VAC irrigation was used to clear the infection. All the metalwork was removed and replaced with circular frame. Patient was put on prophylactic antibiotics after discussion with microbiology consultant. Bone defect was again filled with the bone cement mixed with a bone substitute loaded with antibiotics. Non-union of proximal tibia was still present.

Two-level TSF frame with “clickers” distally for callus distraction.

Front view X-ray of the same leg and on the picture on your left hand side.

Side view with fracture defect on proximal tibia visible and corticotomy on the distal tibia just above one ring before last.
After the infection settled subtotal removal of bone cement was done, one broken olive wire was removed and replaced with two olive wires. Distal tibial corticotomy was done using a drill-bit and an osteotom (low energy corticotomy) and distraction osteogenesis will start next Wednesday, 9 days post corticotomy. “Clickers” which were already included in the original frame will be used to lengthen the leg back to the length after the docking of the proximal non-union will cause leg to shorten in my estimate for around 5 cm. Corticotomy will also increase the blood supply in the area.
Current plan is:
- Docking the proximal fragment into the medullary canal of the distal fragment using TSF and shortening the leg
- Lengthen the leg distally to compensate for previous shortening but also shortening caused by compressing proximal non-union (my estimate 6-8 cm which will take 3 months of bone to grow).