I find it extremely difficult to adjust the fine wire frame in tibio-calcaneal fusion. Whilst I have gotten lucky quite a few times in the past, recently I failed twice. Dramatically. This kind of event puts me down quite badly and makes me feel rather incompetent but I cannot even imagine how patients feel. On top of the pain and discomfort, they are all faced with prolonged treatment – more time with a ****** cage on their leg.
My strategy so far was to aim and adjust the frame based on X-rays in lateral position and based on clinical examination for the AP correction (translation and valgus). Quite often I see that X-ray of an ankle joint in the AP view is not very clear and inter-/intra-observer variability must be quite significant (never tested it myself but I expect it is). The fact is, I don’t know what I am aiming at in relation to an AP ankle X-ray.
I looked at the available options.
- CT scan – high radiation dose, not readily available in clinical settings.
- Tomography – due to the circular structure of the frame, artefact from the metalwork makes bone shadow almost unrecognisable.
I cannot find any other imaging options, and particularly none which would be readily available to me in the clinic.
Analysing the problem again I realised that my main problem is not being able to see the target. Possible solutions:
- always the same AP and lateral views of the ankle – this is very likely possible but with radiographers changing regularly it is probably very difficult to achieve it. I was still left with the original problem what represents my target in AP view of the ankle joint,
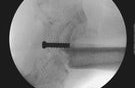
- marking the target – this seemed like a very sensible idea but the question of what to use for a marker arises. Ideally, I was thinking about something reabsorbable or something we can later remove easily. Until today I couldn’t find any reasonable options and decided to use 6.5mm cannulated cancellous screw.
Cancellous screw as a target marker
It is obviously visible on any X-ray unless covered by the frame, but it needs to be surgically inserted through the sole of the foot creating a scar on the weight bearing area. Not ideal, but in the absence of any better solution I will have to accept it as even worse than a scar on the sole of a foot is another failed tibia-calcaneal fusion.